gm blog 18/04/2023 of a 29yr old female patient
This is an online E-log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
 icterus- absent
icterus- absent








This E log book also reflects my patient centered online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and prognosis
A 29 yr old female residence of gurrampudu nalgonda district came with
Cheif complaint: she came to gynaecology OPD 4days ago for tubectomy and diagnosed with severe anemia and reffered to general medicine
She had fever 2days ago and complaints of weakness
History of presenting illness:
Patient was apparently asymptomatic 2 days ago and then developed fever which is sudden in onset,low grade And intermittent type not associated with chills and rigors relieved on medication and no aggravating factors present.
She had generalised weakness since 2 days while doing daily routine works.
H/o bleeding for 7 days last month without clots and normal flow.
No H/o pain abdomen,
No H/O cough,cold and headache
No H/O burning micturition
No H/O weight loss,loss of appetite.
No H/o blood in stools,melena
Menstural history:
Age of menarche: 15 years
Regular cycle of 30 days with 5days bleeding till February
Last month she had bleeding for 7 days with normal flow without clots
Past history:
She is not a known case of diabetes, hypertension, tuberculosis,asthma,epilepsy and thyroid disorders.
No h/o medication
No h/o blood transfusions
H/o of 2 cesarian sections
Family history: not significant
Personal history:
Diet: mixed
Appetite: decreased
Sleep: adequate
Bowel and bladder movements: regular
Addictions: none
General examination
Patient is conscious, coherent and we'll oriented to place and time
Thinly built and malnourished
Pallor - present
Cyanosis-absent
Clubbing- Absent
Koilonychia- absent
Lymphadenopathy - absent
Oedema - absent
Vitals
Temperature- febrile on touch
Blood pressure- 110/70
Pulse Rate-80 BPM
Respiratory rate- 20 cpm
Systemic examination
CVS EXAMINATION:
Inspection :
Shape of chest- elliptical
No engorged veins, scars present
Trachea position central
Jvp- normal
Apical impulse- present
Palpation :
Trachea - central
Apex beat can be palpable in 5th inter costal space
No thrills and parasternal heaves can be felt
Percussion:
All boarders of heart are felt.
Auscultation :
S1,S2 are heard
no murmurs
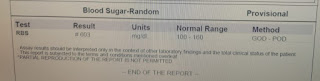
Investigations
Provisional diagnosis: iron deficiency anemia
TREATMENT:
10 PRCB transfusion
Tab dolo 650mg
Tab.ferrous ascorbate+folic acid
Comments
Post a Comment